.png)




.webp)
A nurse practitioner can open their own practice, but the path depends on your state's practice authority designation. In full practice authority states, NPs can evaluate patients, diagnose conditions, prescribe medications, and run an independent practice without physician oversight. In reduced or restricted practice states, a collaborative practice agreement with a physician is required. As of 2026, 27 states and Washington D.C. grant full practice authority.
TL;DR - Can a Nurse Practitioner Open Their Own Practice? 9 Essential Steps for Success in 2026
- Opening an independent NP practice is possible in all 50 states, but what it looks like depends on your state's practice authority designation. Full practice authority states allow complete independence; reduced and restricted states require some level of physician collaboration or supervision.
- The regulatory landscape is moving quickly: 23 states enacted APRN legislative or regulatory changes in 2025 alone. Verifying your state's current designation through the AANP or your state nursing board is a necessary first step before any planning begins.
- The pre-launch phase typically takes six to twelve months at minimum. Core tasks include practice authority verification, DEA registration, business planning, insurance credentialing, and team building — all of which need to be completed before you open, not after.
- Under-capitalization is the most common reason NP practices fail in their first two years. Most advisors recommend reserving 12 to 18 months of operating expenses before launch, and startup costs consistently run higher than first-time practice owners anticipate.
- The market conditions in 2026 are favorable, with 46% NP employment growth projected through 2033 and physician shortages deepening across primary care. Whether the opportunity is right for you depends on your state's regulatory environment, your financial readiness, and whether there is genuine patient need in your intended practice location.
- Still completing your clinical rotations? Create your free NPHub account to find a vetted preceptor and keep your graduation timeline on track.
What It Actually Takes to Open Your Own NP Practice
At some point, the idea of opening your own practice stops being abstract. Maybe you've spent years working under physician oversight in a system that wasn't built around your patients' needs. Maybe your state recently expanded full practice authority and the barrier you've been waiting on just dropped. Whatever the moment was, you're now asking a practical question: what does it actually take to open an NP practice and make it work?
This guide walks through nine factors every nurse practitioner needs to understand before launching an independent practice, from practice authority and startup costs to team structure and the business decisions that determine whether a private practice survives its first two years. The goal is not to inspire you. It is to give you an accurate picture of what the process involves so you can make a clear-eyed decision about whether now is the right time and how to move forward if it is.
Your clinical training prepared you to evaluate patients, prescribe medications, and deliver comprehensive care. Running a nurse practitioner practice requires a separate layer of decisions, and those are what this guide covers.
1. Understanding the Challenges and Setting a Strong Foundation
Most nurse practitioners who open their own practices are clinically ready long before they are operationally ready. That gap is where most early-stage NP practices run into trouble. Understanding what the transition actually involves, before you commit resources to it, is the first factor that separates practices that sustain from ones that close within two years.
Medical practices require significant initial investment, and that is especially true for solo practitioners and small primary care providers. The American Association of Nurse Practitioners notes that while full practice authority states offer more flexibility in how an NP practice can be structured, the operational challenges exist regardless of your state's practice designation. The financial and staffing realities do not change because you have autonomy. They change because you no longer have an employer absorbing them.
The core financial considerations every NP should account for before launch include:
- Equipment and office space: Physical exam equipment, diagnostic tools, and a compliant clinical space represent the largest upfront costs for most new practices.
- Malpractice insurance: Coverage requirements vary by state and specialty, but this is a non-negotiable cost that needs to be built into your budget from day one.
- Technology infrastructure: EHR systems, billing platforms, and tools for interpreting diagnostic tests require both upfront investment and ongoing maintenance costs.
- Working capital: Most practice advisors recommend reserving 12 to 18 months of operating expenses before opening, because revenue rarely covers costs in the early months.
Beyond finances, the team you build in the first phase of your practice directly determines how much of your time goes to patient care versus administration duties. The essential roles to plan for include:
- A collaborating physician: Required in reduced and restricted practice states. Even in full practice authority states, some NPs choose to maintain a collaborative relationship for complex cases.
- An office assistant: Someone to handle scheduling, intake, and day-to-day administration duties so those tasks do not fall to you by default.
- A billing specialist: Medical coding is not covered in most NP programs, but it is one of the highest-leverage hires you can make. Improper coding is one of the most common reasons NP practices lose revenue they have already earned.
- Legal and financial counsel: An attorney familiar with practice regulations and an accountant who understands healthcare operations are both worth the cost before you sign anything.
Dr. Mariea Snell, DNP, APRN, FNP-C and founder of Provider Skills, puts it plainly: "Find expert medical coding specialists. While nursing practice focuses on comprehensive care, your ability to sustain your practice depends on proper coding and billing. This isn't taught in most NP programs, but it's essential for practice success."
Before moving to the next phase of planning, work through these three action steps:
- Audit your state's requirements: Confirm your practice designation, nurse practitioner scope of practice, and whether a collaborative practice agreement will be required.
- Start building your support network: Identify potential medical assistants, billing specialists, and collaborating physicians before you need them. These relationships take time to establish.
- Map your operational gaps: Be honest about which parts of running a business you are not equipped to handle alone, and plan to hire for those gaps rather than absorb them yourself.
The practices that struggle earliest are usually the ones where the NP is trying to cover clinical, administrative, billing, and compliance responsibilities simultaneously. A skilled team does not just support your practice. It is what makes sustained patient care possible.
2. Understanding Your State's Practice Authority: A Critical First Step
Your state's practice authority designation is not a background detail. It is the foundational variable that determines what your NP practice can look like, how it must be structured, and what it will cost to operate. Before any other planning begins, you need to know exactly where your state stands and what that means for your specific situation.
Practice authority in the United States falls into three models, and the differences between them have direct implications for how you treat patients, prescribe medications, and whether you are required to maintain a formal relationship with a collaborating physician.
- Full practice authority: NPs in these states have complete autonomy to evaluate patients, diagnose conditions, prescribe medications, and establish independent practices without physician oversight. As of 2026, 27 states and Washington D.C. operate under this model, and the number continues to grow as state legislatures respond to physician shortages and primary care gaps.
- Reduced practice authority: These states allow NPs to practice with some independence but require a collaborative practice agreement with a physician for certain functions. The scope of what requires collaboration varies by state, so the practical impact on your practice depends on your specialty and the services you intend to offer.
- Restricted practice authority: NPs in restricted states must practice under physician supervision and face the most significant limitations on prescribing authority and independent operation. Opening a truly independent practice in a restricted state is either not possible or requires a formal supervisory structure that adds cost and operational complexity.
Knowing your state's model is the starting point. Staying current as regulations evolve is an ongoing responsibility. Practice authority legislation has been moving quickly, and a state that required physician supervision two years ago may look different today. The most reliable sources for tracking these changes are:
- The American Association of Nurse Practitioners (AANP): Publishes updated state practice environment maps and legislative tracking for NPs across all 50 states.
- Your state nursing board: Issues formal guidance on scope of practice, prescribing authority, and any new requirements tied to recent legislation.
- Your state's NP association: Often the fastest source of practical, on-the-ground information about how new regulations are being implemented and what they mean for practicing NPs.
Understanding your practice authority designation is not a one-time task. It is an ongoing part of operating responsibly as an independent NP.
3. The Expansion of Full Practice Authority in 2026
The regulatory landscape for nurse practitioners continues to move, and legislation produced more legislative activity than most years before it.
According to the 38th Annual APRN Legislative Update, 23 states enacted legislation and/or regulatory changes pertaining to APRN practice, covering everything from full practice authority expansion to prescriptive authority changes and administrative modernization. For NPs evaluating whether to open an independent practice, that momentum has direct operational implications.
The three-tier practice authority model still governs how NP practices can be structured across the country, and where your state lands determines what your independent practice can legally look like:
- Full practice authority: NPs in these states can evaluate patients, diagnose conditions, prescribe medications, and operate an independent practice without physician oversight or a collaborative practice agreement. The AANP tracks this designation state by state, and the number of FPA states has grown steadily as physician shortage data continues to strengthen the policy case for APRN utilization.
- Reduced practice authority: These states allow NPs to practice with some independence but require a collaborative practice agreement with a physician for certain functions, most commonly prescribing. The scope of what requires collaboration varies by state, and some states have established transition-to-practice hour requirements that lead to full independence after a set period.
- Restricted practice authority: NPs in restricted states must practice under physician supervision and face the most significant limitations on prescribing authority and independent operation. Opening a truly independent NP practice in a restricted state is either not possible or requires a formal supervisory structure that adds cost and complexity.
Several legislative developments are worth noting for NPs in specific states. Wisconsin passed a bipartisan bill granting CNPs, CNSs, CNMs, and CRNAs eligibility for independent practice after completing 3,840 hours of professional nursing practice over at least 24 months and 3,840 hours of APRN practice under physician collaboration, with the new law taking effect September 2026.
In Oklahoma, a pathway to independent prescriptive authority was established, allowing CNPs, CNMs, and CNSs to apply to prescribe Schedule III-V controlled substances independently after completing 6,240 clinical hours under physician supervision, effective November 1, 2025. Washington D.C. also expanded independent practice authority under HORA 2024.
The pace of change is accelerating: with about half of respondent states enacting changes in a single year, the regulatory landscape is evolving more rapidly than in previous decades. For NPs planning an independent practice, this means two things. First, your state's current designation may not reflect what was true two years ago, so verifying current status through the AANP or your state nursing board is a necessary first step, not a formality. Second, if your state is in the reduced or restricted category today, that may not be the permanent reality.
Three action steps worth taking before moving forward with any practice planning:
- Confirm your state's current designation: Use the AANP's state practice environment map and cross-reference with your state nursing board's current regulations. Legislative changes can take effect on specific dates, and what applied when you last checked may have changed.
- Track pending legislation in your state: Your state NP association is typically the fastest source of real-time information on bills moving through the legislature and what those changes mean practically for NPs planning independent practices.
- Assess your community's primary care landscape: Practice authority creates the legal opening. Whether there is a patient population that needs your services, particularly in underserved areas with limited access to primary care providers, is the market question that determines whether the opportunity is viable.
4. The Timeline: Why Patience Is Critical for Practice Success
Most NPs who open their own practices underestimate how long the pre-launch phase actually takes. The clinical decision to move forward can happen quickly. The operational reality that follows does not. Under-preparation in the pre-launch phase is one of the most consistent reasons early-stage NP practices struggle, and it is almost always a product of compressing a timeline that genuinely requires time.
The pre-launch planning phase typically runs six to twelve months at minimum, and longer if you are navigating a reduced or restricted practice state or credentialing with insurance panels. The core tasks in this phase include:
- Reviewing your practice authority requirements: Confirm your state's designation, whether a collaborative practice agreement is required, and what the prescribing authority process looks like in your state.
- Securing prescribing certification and DEA registration: If you do not already hold these, factor in the application timelines. DEA registration alone can take several weeks, and some states require additional controlled substance registrations on top of it.
- Developing a business plan: This is the document that forces financial projections, patient volume assumptions, and operational decisions to become concrete before you commit resources.
- Credentialing with insurance panels: If you intend to accept Medicare, Medicaid, or private insurance, plan for three to six months from application to active status. Practices that open before credentialing is complete either turn away insured patients or provide services they cannot yet bill for.
- Establishing a collaborative practice agreement if required: If your state requires a collaborating physician, identifying that person and negotiating the agreement takes time. The terms have real operational and financial implications.
Many NPs continue working in urgent care facilities or with primary care physicians during this phase, which maintains income while startup costs accumulate. The consistent guidance from NPs who have been through this process is to give pre-launch more time than you think you need. A practice that opens when the operational foundation is solid has a meaningfully better chance of reaching financial sustainability than one that opens before it is ready.
5. Financial Planning: Building a Strong Foundation for Your Independent Practice
Many nurse practitioners dream of establishing their own practices, but successful private practices require substantial capital investment. Even with $100,000 in savings, most qualified health professionals find they need additional funding to achieve complete autonomy in their practice.
According to Bottom Line Practice Solutions, under-capitalization is the primary reason many nurse practitioner practices fail. This is particularly crucial in restricted practice states where additional overhead for physician oversight may be required.
Essential Startup Costs for NP Practices:
Clinical Requirements:
- Equipment for physical exams and diagnostic tests
- Electronic Health Records (EHR) system
- Medical supplies and inventory
- Malpractice insurance coverage
- Professional licenses and certifications
Operational Necessities:
- Office space lease and renovation
- Medical assistants and office assistant salaries
- Marketing to prospective patients
- Technology for prescribing medications
- Administration duties support systems
Legal and Professional Services:
- Attorney fees for practice regulations compliance
- Collaborative practice agreement costs (if required)
- Business formation and professional license fees
- Accounting and billing systems
- National Provider Identifier registration
Smart Funding Strategies:
- Traditional Funding:
- Business loans specifically for healthcare providers
- Small Business Administration (SBA) loans
- Medical equipment financing
- Working capital lines of credit
- Alternative Options:
- Partnership with established primary care physicians
- Joint ventures with other nurse practitioners
- Medical practice incubators
- Healthcare-specific investors
Your ability to prescribe medication and interpret diagnostic tests means nothing without proper financial backing. To ensure the sustainability of your practice, consider working with a financial advisor who understands healthcare operations and business management.
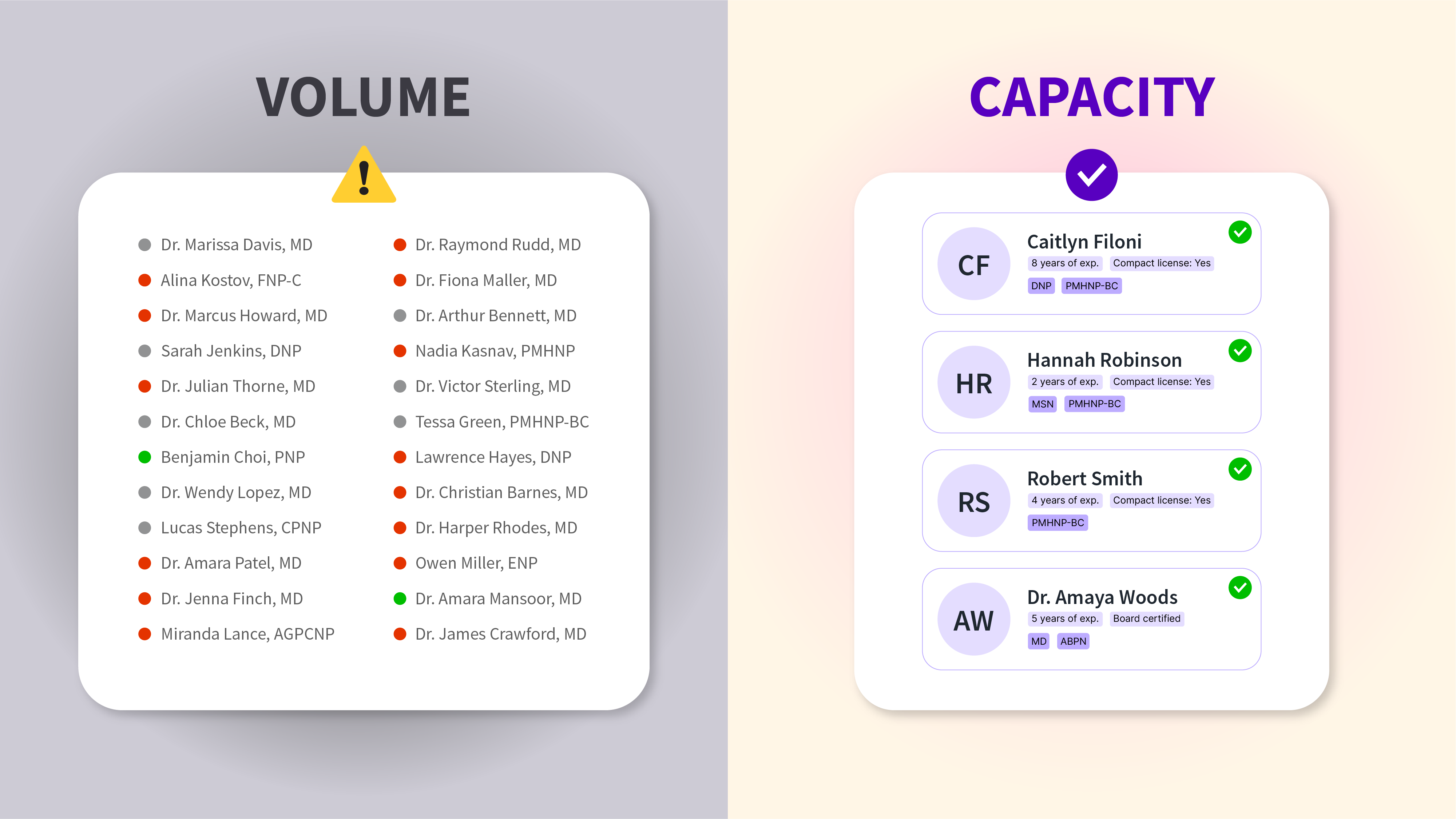
6. Building Your Healthcare Dream Team
The practices that struggle earliest are almost always the ones where the NP is trying to cover clinical, administrative, billing, and compliance responsibilities simultaneously. A well-structured team does not just support your practice operationally. It is what makes sustained, quality patient care possible over time.
The core team structure for an independent NP practice has two sides: clinical and administrative. Both need to be planned before you open, not built reactively as gaps become problems.
On the clinical side, the roles to plan for include:
- A collaborating physician: Required in reduced and restricted practice states. Even in full practice authority states, some NPs maintain a collaborative relationship for complex cases. If your state requires one, this is not a role you can leave open at launch.
- Medical assistants: Handle patient intake, vitals, rooming, and clinical support tasks. Hiring even one qualified medical assistant frees significant clinical time and improves patient flow from the first week.
- Additional NPs or physician assistants: Relevant as your practice grows and patient volume increases. Early-stage practices rarely need additional clinical providers at launch, but building relationships with qualified candidates before you need them saves time when you do.
On the administrative side, the roles that have the most direct impact on practice sustainability are:
- A billing specialist: Improper coding is one of the most common and preventable sources of revenue loss in NP practices. This is not a role to fill with a generalist or to absorb yourself.
- An office assistant: Scheduling, intake coordination, records management, and day-to-day administrative duties need a dedicated owner. When these tasks fall to the NP by default, clinical capacity and patient care quality both suffer.
When evaluating candidates for any role, the practical questions to work through are: how does this hire affect our ability to see and care for patients, what does leaving this position unfilled actually cost in time and revenue, and does this person understand both the patient care mission and the business realities of a small practice.
Two recruitment resources worth using early: your state NP association and local nursing school networks. Both tend to connect you with candidates who understand the NP practice environment and are looking for the kind of work an independent practice offers.
7. AI Tools in Independent NP Practices
AI-assisted tools have moved from experimental to practical in clinical settings, and for independent NP practice owners, they address a specific operational problem: time. In a small practice where the NP is both the primary clinician and one of the key decision-makers, anything that reduces administrative load without adding complexity has real value.
The categories where AI tools are producing measurable impact for independent practices in 2026 include:
- Automated charting and documentation: AI-assisted EHR systems can generate draft clinical notes from patient encounters, reducing the time spent on documentation after each visit. For a solo or small-team practice, this translates directly to more patient capacity or more time outside the clinic.
- Appointment and scheduling management: AI-powered scheduling tools handle routine inquiries, appointment reminders, and follow-up coordination without requiring staff time for each interaction.
- Predictive analytics for high-risk patients: Some platforms now analyze patient data to flag individuals who may need proactive outreach, which supports the kind of preventive, relationship-based care that independent NP practices are well-positioned to deliver.
A few practical considerations before adopting any AI tool: verify that the platform integrates with your EHR system, confirm that data handling meets HIPAA requirements, and evaluate the actual time cost of implementation against the time savings it produces. AI tools that require significant staff training or workflow restructuring can create short-term disruption that offsets their longer-term benefits.
The goal is not to build a technology-forward practice for its own sake. It is to find the specific tools that reduce the administrative burden on you and your team so that the clinical work, the part that sustains the practice, stays at the center.
8. Balancing Patient Care with Business Success
Clinical expertise is what qualifies you to open an NP practice. Business acumen is what determines whether it stays open. Most NPs who struggle with the business side of practice ownership do not lack intelligence or work ethic. They lack exposure to a set of skills that nursing programs do not teach and that clinical experience does not develop.
The transition from clinician to practice owner requires building competency in three areas that operate alongside your clinical work:
Financial management covers the decisions that determine whether the practice is economically viable. This includes developing clear pricing strategies for medical services, understanding how insurance reimbursement models work and where revenue leaks occur, monitoring cash flow against operational expenses on a regular basis, and planning capital allocation for future growth. A practice that delivers excellent patient care but cannot cover its operating costs will not survive long enough to serve anyone.
Operational efficiency covers how the practice runs day to day. Streamlined scheduling protocols, clear procedures for medical assistants, systems for documentation and diagnostic test coordination, and defined workflows for administration duties all reduce friction that otherwise accumulates into lost time and revenue. In a small practice, operational inefficiency has an outsized impact because there is less organizational slack to absorb it.
Strategic planning covers the longer arc: setting realistic patient volume and revenue targets, monitoring your practice location's demographics and community health needs, adapting to changing practice regulations, and making deliberate decisions about scope of services and growth. Practices that grow without a plan tend to grow into problems.
If any of these areas falls outside your existing competency, the right response is to hire for it rather than absorb it. A practice manager with NP practice experience, a healthcare-focused accountant, a billing specialist who understands medical services coding, and legal counsel familiar with practice authority requirements are all positions that pay for themselves in the problems they prevent. The cost of not having them usually shows up in the first year, and by then it is harder to correct.
9. Opportunity on the Rise: The Case for NP Practice Ownership in 2026
The workforce data behind NP practice ownership has strengthened considerably in recent years, and it is worth understanding what that data actually says rather than treating it as background motivation.
The Bureau of Labor Statistics projects NP employment growth of 46% through 2033, making it one of the fastest-growing roles across all healthcare occupations. That growth is driven by a combination of factors that are structural rather than temporary: a deepening physician shortage, an aging patient population with increasing primary care needs, and a healthcare system that has consistently failed to build enough provider capacity in rural and underserved areas. These are not short-term conditions. They are the environment independent NP practices will be operating in for the foreseeable future.
For NPs evaluating whether to open an independent practice, this context matters in a specific way. The demand for primary care services in many communities exceeds current supply, which means a well-positioned NP practice is not entering a saturated market. It is filling a gap that existing providers cannot close.
Three practical considerations for translating that opportunity into a viable practice:
- Identify the specific care gaps in your intended practice location: High NP demand nationally does not mean high demand in every zip code. Research wait times, provider-to-patient ratios, and unmet health needs in your community before settling on a practice location and service mix.
- Align your specialty with local need: Chronic disease management, mental health services, and women's health are consistently high-demand areas across many markets, particularly in communities that have lost primary care providers to retirement or consolidation.
- Consider telehealth as part of your service model: Telehealth expands your geographic reach without proportionally increasing your overhead. For NPs serving rural or underserved populations, it can be a meaningful part of a sustainable practice model from the start.
The opportunity in 2026 is real. Whether it is the right opportunity for you, in your state, in your community, at this point in your career, depends on the factors this guide has covered. The market conditions are favorable. The rest is planning.
Taking the Next Step Toward Independent Practice
Opening your own NP practice is a decision that sits at the intersection of clinical readiness, operational preparation, and market opportunity. The clinical readiness is something you have been building throughout your career. The operational preparation is what this guide has covered. The market opportunity, in 2026, is genuine.
The nurse practitioners who make independent practice work are not the ones who waited until every variable was certain. Certainty is not available in this process. They are the ones who understood the regulatory environment in their state, built their financial foundation before they needed it, assembled the right team before gaps became problems, and gave the pre-launch phase the time it actually required rather than the time they wished it required.
What your independent practice makes possible goes beyond the business case. A confirmed, operational NP practice means your patients have a provider who knows them. It means your community has access to care it may not otherwise have. It means the years you have invested in your clinical training are being deployed at the fullest extent of your scope of practice. That is the outcome that makes the operational work worth doing.
If you are an NP student still working through your clinical rotations and trying to figure out what comes next, NPHub connects NP students with vetted preceptors across specialties and states so you can complete your hours and graduate on schedule. You can create your free NPHub account and start exploring available preceptors today.
FAQ: Opening Your Own NP Practice in 2026
1. Can a nurse practitioner open their own practice without physician oversight?
It depends on your state. In full practice authority states, NPs can open and operate an independent practice without physician oversight or a collaborative practice agreement. In reduced and restricted practice states, some level of physician involvement is required. Confirm your state's current designation through the AANP or your state nursing board before any planning begins.
2. What states allow nurse practitioners to practice independently in 2026?
The AANP maintains an updated state practice environment map that tracks full, reduced, and restricted practice states. As of 2026, the regulatory landscape is moving quickly, with 23 states enacting APRN legislative or regulatory changes in 2025 alone. Check the AANP map directly for the most current state-by-state breakdown.
3. How much does it cost to open an NP practice?
Startup costs vary significantly by state, specialty, and practice size, but most practice advisors recommend having 12 to 18 months of operating expenses in reserve before opening. Core costs include equipment, EHR systems, malpractice insurance, office space, staff salaries, and legal and billing setup. Under-capitalization is consistently cited as the primary reason NP practices fail in their first two years.
4. Do I need a collaborative practice agreement to open my own practice?
Only if your state requires one. In full practice authority states, no collaborative practice agreement is needed. In reduced practice states, a formal written agreement with a collaborating physician is required for certain functions, most commonly prescribing. In restricted practice states, physician supervision is mandatory. Your state nursing board is the authoritative source on what your specific situation requires.
5. How long does it take to open an independent NP practice?
The pre-launch phase typically runs six to twelve months at minimum. Key tasks include confirming practice authority requirements, securing DEA registration, developing a business plan, credentialing with insurance panels, and securing office space. Insurance credentialing alone can take three to six months. NPs who try to compress this timeline consistently run into problems that could have been avoided with more preparation time.
6. Can a nurse practitioner prescribe medications independently?
In full practice authority states, yes. NPs in these states have independent prescribing authority, including for controlled substances, without physician delegation or oversight. In reduced and restricted practice states, prescribing authority is either limited or requires physician collaboration. Some states have established transition-to-practice hour requirements that lead to independent prescribing authority after a set period of supervised practice.
7. What licenses and certifications do I need to open an NP practice?
At minimum you will need an active RN license, national board certification in your NP specialty, a state APRN license, DEA registration if you intend to prescribe controlled substances, a National Provider Identifier, and a business entity registration. Some states require additional controlled substance registrations on top of federal DEA registration. If your state requires a collaborative practice agreement, that must be in place before you see patients.
8. What is the difference between full, reduced, and restricted practice authority?
Full practice authority means NPs can evaluate patients, diagnose, prescribe, and operate independently without physician oversight. Reduced practice authority allows NPs to practice with some independence but requires a collaborative practice agreement with a physician for certain functions. Restricted practice authority requires physician supervision and imposes the most significant limitations on independent operation and prescribing. The AANP defines and tracks these designations for all 50 states and Washington D.C.
9. How do nurse practitioners get reimbursed by insurance in private practice?
NPs bill under their own National Provider Identifier and can receive direct reimbursement from Medicare, Medicaid, and most private insurers. Reimbursement rates vary: Medicare reimburses NPs at 85% of the physician rate, while Medicaid rates vary by state, with some states reimbursing at 100% of the physician rate. Credentialing with each payer panel is required before billing, and that process typically takes three to six months per payer.
10. Is 2026 a good time to open an NP practice? The market conditions are favorable.
The Bureau of Labor Statistics projects 46% NP employment growth through 2033, physician shortages are deepening, and full practice authority continues to expand across states. Whether it is the right time for you specifically depends on your state's practice authority designation, your financial readiness, and whether there is a genuine patient need in your intended practice location. The opportunity exists. The planning determines whether you are positioned to act on it.
About the Author
- NPHub Staff
At NPHub, we live and breathe clinical placements. Our team is made up of nurse practitioners, clinical coordinators, placement advisors, and former students who’ve been through the process themselves. We work directly with NP students across the country to help them secure high-quality preceptorships and graduate on time with confidence. - Last updated
Jun 2, 2026 - Fact-checked by
NPHub Clinical Placement Experts & Student Support Team - Sources and references
Find a preceptor who cares with NPHub
Book a rotation.webp)

.webp)

%20(3)%20(2).svg)